


The Life Long Medicalization of the Trans-identifying Patient
Even if you don't detransition, you're on the medical leash for life...

Most people can't consider what it means to be a life-long medical patient, but for trans-identifying people who choose to medically transition, this is the reality. For detransitioners, the damage, both physical and mental, is worse, but even if you don't detransition, you will spend the rest of your life going to the doctor, taking medicine, and having surgery.

The above is a comment I received on my Twitter from a trans-identifying male, proclaiming proudly that they will be seeing a doctor over and over.
Gender Affirming Care
What is gender affirming care? Well, it's quite the opposite of what it sounds like. It is the process of denying the natal sex to affirm a belief that the patient, suffering from gender dysphoria, is the opposite sex. The first procedure to happen is the changing of the mind. Medical procedures are done to affirm the opposite sex identity, including puberty blockers, cross sex hormones, and surgery.
Cross sex hormones will be taken by the patient for the rest of their life to affirm the identity. They become necessary for health after prolonged hormone abuse or after surgery. Extended use of wrong sex hormones causes the inability to create ones own hormones, thus dependency. Stopping the use of hormone replacement therapy has not been studied and could be extremely dangerous.
As for surgeries, these is usually more than one, and the results are permanent. Top surgery, the removal or addition of the breasts, has less complications than bottom surgery, which is heinous for both sexes. Top surgery can still be very traumatic, and takes lots f recovery time. Bottom surgery usually consists of multiple surgeries and revisions have to be made more often than not.
Puberty Blockers
Puberty blockers stop and end the natural puberty of a trans-identifying child and arrests their development. The most commonly used drug is Lupron, an anti-cancer drug previously used to castrate pedophiles. Puberty blockers are usually followed by cross sex hormones when the child reaches the natural age of puberty, and this combination always leads to sterilization and the inability to orgasm.
Puberty blockers stunt brain growth and interrupt bone growth, causing decreased IQ and early osteoporosis. Once the time for natural puberty has passed, there is no way to go back and start it again. All of the development that was lost is gone forever. Time is not reversible. This includes development of the brain, bone density, immune system, and genitals, all of which will be stunted by puberty blockers. Mood disorders can occur from the side effects and the interrupted brain development, as well as cognitive delays and damage.
“Emotional instability” is on the box as a warning for Lupron. Puberty blockers can cause depression, anxiety, irritability, and suicide-related symptoms. This goes in direct conflict with the claims that puberty blockers relieve distress and reminds us of the suicide myth. Of course, trans-identifying people are more likely to commit suicide after receiving gender affirming care. (But why?)
Wrong Sex Testosterone
Women who identify as men are given enough testosterone to raise their levels 10-40 times above the healthy, average female reference range. The goal of providers is to raise the levels of testosterone to those of a male their age and weight. The female body was not built to handle the severe side effects that follow.
The FDA has not approved testosterone for use in trans-identifying females. On this bottle, it says, “WARNING: Not for use in women.” Testosterone is a carcinogen, causing cancer in the female reproductive system. It causes cancer in the uterus, ovaries, cervix, and breasts. This is why, when you start wrong sex testosterone, your doctor will tell you that a complete hysterectomy may be in your future. Before cancer develops, however, ovarian cysts can be expected, as well as irregular, painful periods, endometriosis, and more. For me, the atrophy was to severe that my uterus is folded over now. I detransitioned before I had it removed. I did have my breasts removed, however.
Everything that happens to the outside of a woman's body, the growth, expansion, and redistribution of muscle and fat, happens on the inside, too. This means that it's not only her shoulders and back getting larger, but her larynx will grow, and subsequently will be crushed in her throat, and her heart will grow, too, which will increase the likelihood of a heart attack by a rate 2x than that carried by men. That's 4x the rate of the average female.
Testosterone also affects blood sugar and can lead to the development of type 2 diabetes. It can cause high blood pressure, sugar, and cholesterol, all of which can be a significant health risk. It also increases the risk of blood clots, which can easily occur in deep veins and in the lungs. It also increases risk of stroke.
Wrong sex testosterone can also cause a woman to develop sleep apnea, which can be deadly. Sleep apnea is a condition in which the sufferer periodically stops breathing in their sleep.
Many trans-identifying men report a stunted ability to emote outside of anger and aggression when on testosterone. It takes away the ability to cry and increases impulsivity, increasing the suicide risk once again.
Wrong Sex Estrogen
Similar to trans-identifying men, males who identify as women are given abnormally high levels of estrogen, as well as androgen blockers, when they medically transition. After social transition, which disrupts the mind, the patient is put on these hormones as well as the hormone blockers whose effects also have not been studied on men.
Like testosterone, estrogen use increases the risk for heart attack, blood clots, and stroke. Another serious risk for trans-identifying women is dementia. Did you know, by the way, that when such patients get dementia, they most often revert back to their original male sex and are extremely disturbed by being unable to recognize themselves..?
Estrogen, just like wrong sex testosterone, affects the mood. It can cause mood swings and depression, worsening the comorbidities that trans-identifying people often have. It also causes tiredness, weakness, and chronic fatigue. Cross sex estrogen also has a great impact on sexuality and sexual function. It can take away the ability to create healthy sperm, get an erection, and disregulate the sex drive.
Estrogen taken by men also causes the redistribution of muscle and fat. It usually causes weight gain, which comes along with hot flashes, too. Wrong sex estrogen has also been linked to memory loss and other cognitive issues.
Estrogen in men has many neurological effects which have not been studied, but which we can see in reports from transitioned and detransitioned men. I know one detransitioned man, Abel Garcia, who is suffering from tremors on the left side of his body and is losing the sight in his left eye since beginning cross sex estrogen. No doctor is willing to help him.
Males who take high levels of estrogen are also likely to experience the thinning of their bones. Osteoporosis is a serious disease, and it cannot be reversed.
Chasing the Dragon
Once you start, it's hard to stop. Testosterone and estrogen are hormonal drugs, of course, and they always are dosed with a healthy serving of love-bombing from the trans community. Love-bombing is the narcissistic cult tactic of showering someone with love, affection, and praise in such a way that they become addicted to and dependent upon it.
With every step a trans-identifying person takes towards medicalizing themselves forever, they are worshipped. They are praised. They are love-bombed. This begins a vicious cycle of addiction and dependency. The patient needs to be constantly affirmed by others to feel validated in their chosen sex, and love bombing creates an insatiable need for more.
On top of this, people who identify as trans, especially children, believe that they are sick, “born in the wrong body,” and that hormones are surgery will fix all of their problems.
Is there physical addiction, as well as the addiction to the external validation? Yes. When you first start puberty blockers or cross sex hormones, you get euphoria.
You just got your way. Trans care is entirely patient lead, and you were able to tell your doctor what you wanted and successfully get it.
You're told you're saving your own life. They call it “life saving medicine.” Doctors tell you that you will kill yourself without it. You think you are going to be cured.
Love bombing. It's addicting and it's intense. You begin to need it to feel validated and “affirmed.”
These are the reasons for the temporary euphoria, on top of the actual acute side effects of such strong drugs. For a short time, testosterone is known to cause confidence and estrogen produces a brief soothing effect. But it doesn't last.
After the euphoria from the initial step wears away, you need something new. Eventually, it does go, leaving you in withdrawal, and desperate to feel okay again. This is why, after starting puberty blockers, children almost always move on to hormones, and hormones are then followed by surgery. You are convinced that the happiness wore away because you still aren't “affirmed and aligned” in the “right body,” and straight down the path to life long medicalization you go.
Top Surgery
The next step after hormones.
“Top surgery,” either a radical double mastectomy or breasts implants in a male chest, usually follows the hormone prescription. However, those are those who have been known to have been given surgery before hormones. Some people will say that you have to be in therapy and on hormones for a certain amount of time before being given surgery, but this is false.

Here is a screenshot of a pinned tweet on a trans activist's account, glad to have found doctors that require no therapy before giving gender affirming care. It is an interactive, constantly updated map, giving children and mentally ill people access to drugs and surgery with no therapy.
Both of these surgeries, but especially the double mastectomy, are irreversible.
For a male who gets breast implants, he will have to get the breast implants checked and replaced every few years. If he wants to restore his original, masculine chest, he will have to remove the implants, as well as the extra stretched skin, and will be numb and have scars forever.
For the female, the surgery is nothing short of horrific. All of the healthy mammary tissue is removed, as well as the extra skin. During this time, the nipples, which have been drawn on where they will be cut to create a masculine look, are sliced and reshaped. The nipple bud is cut in half, and the areolas are greatly reduced. Then the nipples are frozen, while the cheat is scraped, before the new nipples are sewn onto the bleeding wound.
If a trans-identifying man chooses to detransition, there is no going back. She will never be able to feed her children, or have her healthy breasts put back. Instead, she can have a breast reconstruction, which consist of at least three surgeries. There has to be a surgery to stretch the skin to make up for what was lost. Tissue expanders will be placed in the chest for at least 6 months before they implants can be put in. A third surgery is needed if she wants her nipples to at least be in the right place again. This is because the nipples are places a masculine, east-west position, during the initial surgery. Nipple grafting has a high failure rate the first time you do it, and is even less likely to be successful if you try again.
Bottom Surgery
Bottom surgery is usually the final step in a gender transition. Or at least it used to be, before more surgeries were invited to help patients continue to chase the dragon. More on this later.
Bottom is the full castration and de-sexing of the patient. It is impossible to change sex, so this is all it is.
During winter procedure, the genitals are mutilated and destroyed and replaced by a wound that constantly tries to heal itself. The body knows that this is wrong, and will fight against the surgery, in most cases, forever.
Trans-identifying males get vaginoplasty. This is the complete removal of the penis and testicles, which removes the ability of the man to make any hormones at all, causing them to be completely reliant on synthetic hormones for life. A small hole is created and the patient is told to “dilate.”
What is dilation? It is the prescription for a rod, which is impaled into the neo-vagina multiple times a day, to prevent it from healing and closing up. In worst case circumstances, the wound heals in pockets, creating a petri dish inside the body which can lead to sepsis. Dilation is completely necessary, and in almost every case, patients will have to do this for the rest of their lives. This is another example of life long medicalization.

These are the large dilation rods used by men who have undergone vaginoplasty.
There are two options for trans-identifying men: phalloplasty and metoidioplasty. Phalloplasty is the most common option. During metoidioplasty, the enlarges clitoris, which is painful, sensitive, and grows with testosterone use, is the pseudo-phallus. In phalloplasty, a “flap,” often coming from the arm, thigh, and less commonly the stomach, is removed and folded into a “penis.” Urethral hookup happens in the months following. This is another multi-surgery for females, adding to the pockets of doctors.
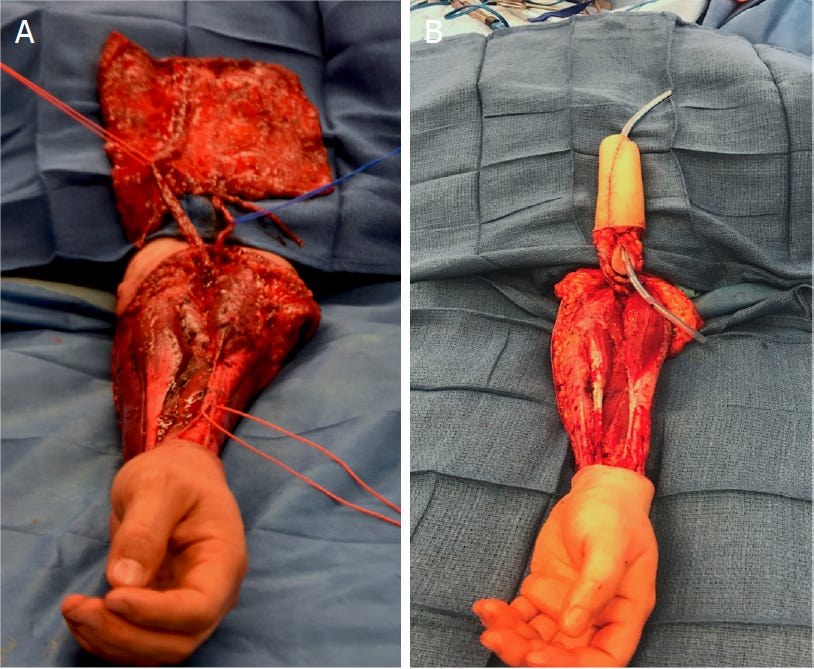
This is the skin and muscle being removed from a female’s arm in an attempt to create the new penis. A catheter is used at the beginning, before the following surgeries are performed.
Phalloplasty complications include rejection, inability to urinate or complete urination, infection, unsightly scarring, granulation tissue formation, decreased mobility, hematoma, pain, and decreased sensation.
After surgery for either sex, there is a great chance of losing the ability to orgasm, if it was not already lost.
The Other Surgeries
As mentioned earlier, more surgeries have been invented to help patients chase the high. These surgeries include but are not limited to; foot size reduction, clavicle shrinking, hair line surgery, facial feminization surgery, facial masculinizing surgery, adams apple shaving and reduction, adams apple enhancement, and more. There are also hair transplants, surgeries to increase or reduce the hips and butt, and lazer hair removal is another one. More procedures will be invited for this billion dollar industry, and children and the mentally ill will pay the price.
Sources:
Puberty Blockers:
https://acpeds.org/transgender-interventions-harm-children
Testosterone:
https://www.google.com/search?q=fda+testosterone&oq=fda+testosterone+&aqs=chrome..69i57.3744j0j9&client=ms-android-tmus-us-revc&sourceid=chrome-mobile&ie=UTF-8
https://www.mayoclinic.org/healthy-lifestyle/sexual-health/in-depth/testosterone-therapy/art-20045728
Estrogen:
https://www.google.com/search?q=trans+women+dementia&oq=trans+women+dementia+&aqs=chrome..69i57.5725j0j7&client=ms-android-tmus-us-revc&sourceid=chrome-mobile&ie=UTF-8
https://www.cancerresearchuk.org/about-cancer/treatment/hormone-therapy/side-effects-men
Vaginoplasty:
https://www.mtfsurgery.net/dilation.htm
https://www.mayoclinic.org/vid-20517182#:~:text=You%20will%20need%20to%20do,be%20able%20to%20be%20reversed.
Phalloplasty and metoidioplasty:
https://www.google.com/url?sa=t&source=web&rct=j&url=https://www.childrenshospital.org/sites/default/files/media_migration/c81bcb62-cfee-4927-bd6e-f0231cfdb691.pdf&ved=2ahUKEwiq8MedgPv9AhUsoWoFHXx9CpgQFnoECBgQBg&usg=AOvVaw0QaO48bED59G2iOoayHYRO
It is great that you included photographs of the horrors. These horrors should be seen for what they are, and not merely referred euphemistically as "bottom surgeries."
A couple of related points. When the Times published their long article on puberty blockers, "They Paused Puberty, but Is There a Cost?", one of the people who wrote a letter to the Times was Mark Garnick (se his profile here: https://www.dfhcc.harvard.edu/insider/member-detail/member/marc-b-garnick-md/), "one of three academic principal clinical investigators of studies that led to the initial F.D.A. approval of Lupron for the treatment of metastatic prostate cancer," as he wrote in his letter (https://www.nytimes.com/2022/11/28/opinion/letters/puberty-blockers-transgender-youths.html). He went on to state: "...having studied this class of drugs, which includes puberty blockers, for more than four decades...I can say that physicians are still learning and continue to be concerned about the safety of these agents in adults...Woefully little safety data are available for the likely more vulnerable younger population. Bone loss in adult men who have been on these agents is significant, and a leading cause of morbidity with long-term administration...Other safety issues include cognitive, metabolic and cardiovascular effects, still under intense investigation. The prudent and ethical use of such agents in the younger population should demand that every pubertal or pre-pubertal child be part of rigorous clinical research studies that evaluate both the short-term and longer-term effects of these agents to better define the true risks and benefits rather than relying on anecdotal information."
Also, reading the account of Abel Garcia, I was reminded of my conversation with a 70-year-old male detransitioner, and I put it up here: https://mungeribabu.substack.com/p/my-conversation-with-hank. He too is in the process of losing his eyesight in one eye. With the other, he has had repeated retinal detachments. And he mentioned that he knows several MtF detransitioners who suffer from the same problem - retinal detachment. And the list of diseases he suffers from! Several heart attacks (the first one before 40), hypertension, rheumatoid arthritis, scleroderma, low back pain, allergies, asthma, retinal detachment in one eye and loss of sight in another, and a cocktail of medication for his heart. He has had stones in his liver ("the doctors had never seen anything like that"), kidney, gallbladder, and saliva ducts ("the size of lime pits, and they had to operate inside my mouth to get them out.").
It might be very instructive if you can find OLDER transgender people who can narrate all the various things they suffer from after the hormones and surgery. It can be a very instructive series.
And here is the issues with estrogen in men I found in the peer-reviewed literature: https://mungeribabu.substack.com/p/estrogen-is-really-bad-for-men.
Thank you for what you are doing.